
Diversion from the criminal justice system: its creation and development
A mechanism of treatment as an alternative to criminal sanctions, or diversion of drug offenders to treatment (elterelés) was added to the Hungarian legal system in 1993 (Pelle and Dénes 2000). From the beginning, it aimed to provide an alternative to criminal sanctions for offenders who possessed small amounts of illicit substances for personal use, and who had admitted committing the offence. These offenders are offered the opportunity to participate in a 6 month treatment or prevention program as an alternative to criminalisation. The program should be completed within 9 months.
For the duration of this diversion program, the criminal procedure is suspended and if the program is completed, the criminal charges are dropped and the criminal procedure ends with no criminal record. This can be defined as a form of quasi-coerced treatment: the offender is given a choice of either taking the criminal sanction or opting for the alternative treatment.
Offenders have to undergo a preliminary status assessment before they can begin their diversion scheme. The assessment is carried out by a psychiatrist, a clinical psychologist, or a general practitioner, with the use of the Addiction Severity Index (ASI) and/or the European Adolescence Assessment Dialogue (EuroADAD), as well as a general medical check of the offenders’ health. Based on the findings of the assessment of their social and health status, offenders can be referred to one of the three types of diversion programmes described below.
1st Type: Treatment of Drug Dependence
If the offender shows symptoms of drug dependence, the person is referred to a continuous treatment program, which can be either outpatient or inpatient and can include medical and/or psychosocial treatment methods.
2nd Type: Other Type of Drug Treatment
This is for those offenders who are not drug dependent but have drug-related health and social problems, with a focus on social reintegration. This also qualifies as a treatment that can be provided by a professional health care institute.
3rd Type: Preventive-consulting
This is by far the most frequent form of diversion, designed for those who are not diagnosed with drug dependence or any major drug-related disorders. This form of diversion, by definition, is not a form of treatment but a form of indicative prevention. Therefore it is not necessarily provided by a healthcare professional. It is prevention for those who are at risk of developing drug problems. The offender can complete these alternative programs at an outpatient drug centre, or other designed service provider, with biweekly individual or group consultation sessions with a counsellor.
The legislation has been amended multiple times since 1993. When the first Orban government came to office in 1998, it restricted access to the alternatives. For four years, only those who were diagnosed with drug dependence by an expert forensic psychiatrist were offered the alternative to punishment. Other offenders were sanctioned by a criminal court. As a result, the number of people prosecuted and sentenced increased significantly, increasing the workload of prosecutors and judges (Pelle and Dénes, 2000). Assessing drug dependence showed great variance in individual drug offenders and was deemed chaotic by many professionals.
The Socialist-Liberal government coalition abolished this restriction in 2002 and provided unlimited access to alternatives to coercive sanctions for all offenders who possessed illicit drugs for personal use. What is more, it offered this option for those offenders who shared these drugs for non-commercial purposes, that is, for collective use (e.g. the typical scenario where people share a cannabis joint with each other). This amendment was deemed unconstitutional by the ruling Constitutional Court in 2004 (54/2004. (XII. 13.)), stating that there is “no right to intoxication”, and the term “collective use” violates the principle of clarity of the law.
In 2008 a joint decree of the Ministry of Health and the Ministry of Social and Labour Affairs (42/2008) created specific procedural rules for the diversion to treatment mechanism, including professional requirements for service providers and supplementary documents for administration. This decree shaped the timeframe of diversion interventions (at least two hours per two weeks for 6 months, total 24 hours).
In 2011 methodological guidelines (Dudits et al. 2011) on the preventive-consulting diversion were published for service providers, based on the findings of a literature review. It established the 5 steps of this intervention:
1) Needs assessment (with structured interview)
2) Individual intervention plan design (together with the client)
3) Individual or group counselling based on the plan (focusing on improving life skills, motivational interviews, changing negative normative beliefs etc.)
4) Monitoring and evaluation
5) Program finalisation
In 2013 the second Orban government introduced a new, more repressive Criminal Code, with several amendments to the drug related provisions, including the diversion scheme. The most important was to introduce a new limitation to the diversion: only those offenders who have not re-offended within two years can be offered the alternative to punishment. This change has mostly affected regular/dependent drug users who have to face criminal sanctions. Relapse is considered by modern addiction science a natural part of recovery. By applying coercive sanctions to punish relapse, it is treated as a failure to fulfil treatment obligations.
In 2018 the new Criminal Procedural Law came into effect, along with some other changes to the diversion scheme. According to the new law, only the prosecutor can make decisions about the suspension of the criminal procedure, and the criminal court can charge the costs of the criminal procedure (e.g. laboratory test of seized substance) to the offender. This amount can reach several hundred Euros.
Since the completely new Criminal Code and Criminal Procedural Law came into force, civil society organisations have been demanding that the government amends the 2008 ministerial decree on the diversion to treatment, adjusting the rules to the new legal environment. To date, the government has not adopted a new decree. Although the use of novel psychoactive substances has increased significantly in the past ten years, the law does not offer the users of these substances the opportunity of diversion. It only applies to substances scheduled as illegal narcotics (kábítószerek). The use and possession of novel psychoactive substances for personal use is an administrative offence.
Evaluation studies
Research published in 2008 analysed the 628 clients of a Budapest-based service provider, the NGO Kék Pont, who were diverted from the criminal justice system and completed their program at the organisation between 2001 and 2005 (Rácz et al. 2008). They found that after diversion was opened to non-dependent drug users in 2003, the rate of their clients who were diverted by the criminal justice system increased from 24 percent to 72.6 percent. According to the addiction severity index test used at the start of the program, more than half of these clients had no problems that demanded treatment. The authors recommended reassessing the diversion to treatment mechanism because it diverts resources from dealing with those with real treatment demand.
A systematic external evaluation of the diversion to treatment scheme was conducted in 2009, with the financial support of the government. In-depth interviews and a questionnaire were used among service providers and clients to examine their perceptions and experiences about diversion. The findings were published in 2010 (Vitrai 2010). The researchers found that most service providers used the combination of different methods during the diversion program, including individual and group counselling, motivational interviews and other psychosocial support. Before the start of the program, 53 percent of clients had not perceived any problems with their drug use. Low motivation of clients was mentioned by service providers as the most significant barrier to success. 80 percent of clients mainly expected to avoid prison by participating in the program. However, clients reported a reduction in their drug use during their participation. Without a follow up, it is uncertain if this reduction was sustained later.
The second evaluation was conducted in 2016 and 2017, focusing on the 16 largest service providers that covered 69 percent of those clients who participated in diversion to treatment in the two years prior to the research (Felvinczi et al. 2018). The research assessed the demographic and other characteristics of clients (e.g. drug use patterns) and the structure and activities of the preventive-consulting diversion programs. According to the findings, the average person who enters diversion to treatment is young (27.9 years old), male, has at least a high school degree, is well integrated in the labour market and is an occasional user of cannabis (less than monthly). Those who failed to complete the program have significantly lower levels of education and a less secure labour market position.
Researchers also analysed the content of preventive-consulting interventions among 14 service providers. The most prevalent goals of diversion highlighted by service providers were abstinence (although this was not defined as a goal in the methodological guidelines), improving life skills, reduction of problem drug use, and prevention of regular drug use. Client satisfaction was measured with the help of a seven-grade scale, where participants could indicate their agreement with eleven positive and six negative statements about the quality of the service. The vast majority of clients perceived the service positively, although half of the clients said they would not use this service voluntarily. 38.5 percent of clients entering diversion reported a significant reduction in their illicit drug use during the diversion, although this was much higher among cannabis users (28.1 percent) than among MDMA and amphetamine users (5 percent). There was no significant change in drug use among those who reported problem drug use and no significant change in perceptions about healthy lifestyle and life skills.
Barriers
Researchers identified the lack of professionally trained service providers as a significant barrier to improving the quality of diversion interventions. The involvement of clients in setting the goals of the intervention contributed to better outcomes. There were more positive outcomes among those clients who were in a more disadvantaged position when entering treatment.
The research identified the institutional barriers perceived by the service providers:
- Lack of information and cooperation among law enforcement officials;
- Lack of flexibility in the timeframe: there are clients who need a more intensive 3 months of work instead of the 24 hours/6 months timeframe;
- The methodological guidelines are outdated and need to be updated and improved;
- The administrative burden of reporting is too much, needs to be improved;
- Funding of diversion services is unsustainable and erratic;
- No methodological support and training.
Recent trends
Diversion from the criminal procedure is the main reason for people to enter treatment in Hungary. This was the case for almost 80 percent (3384 persons) of all people in drug treatment in 2020. This is not the case in in-patient treatment, where the proportion of those diverted from the criminal justice system was only 7.4 percent (8 persons). With outpatient treatment centres the rate is 87.3 percent. There are no other reported forms of treatment available for those in prisons: 100 percent of the 81 persons entering treatment within the penitentiary system were diverted from the criminal justice system. This gap can be partly explained by the greater motivation of those service providers who work with people diverted from the criminal justice system to provide reliable data about their clients. However, there is no doubt that the majority of people entering treatment in Hungary are coerced.
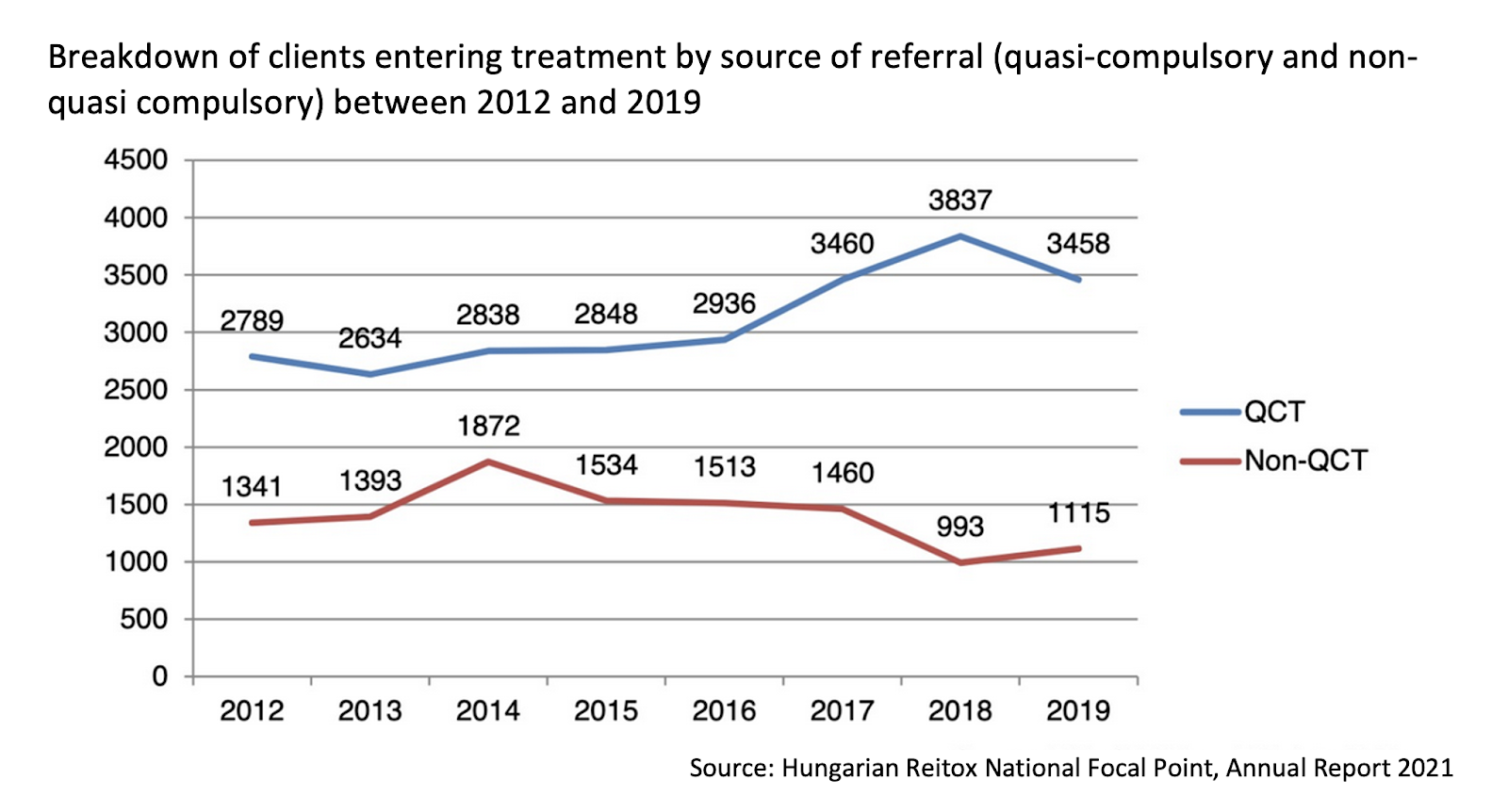
If we look at the trends, we can observe a widening gap between the number of those diverted to treatment and those who enter treatment voluntarily (illustrated by the chart below from the annual report of the Reitox National Drug Focal Point). The rate of diversion was 67 percent in 2012 and the rate of people entering voluntarily was 32 percent. While the number of people entering treatment voluntarily declined from 1341 persons to 1115 persons, the number of those diverted from the criminal justice system increased to 3458 persons.
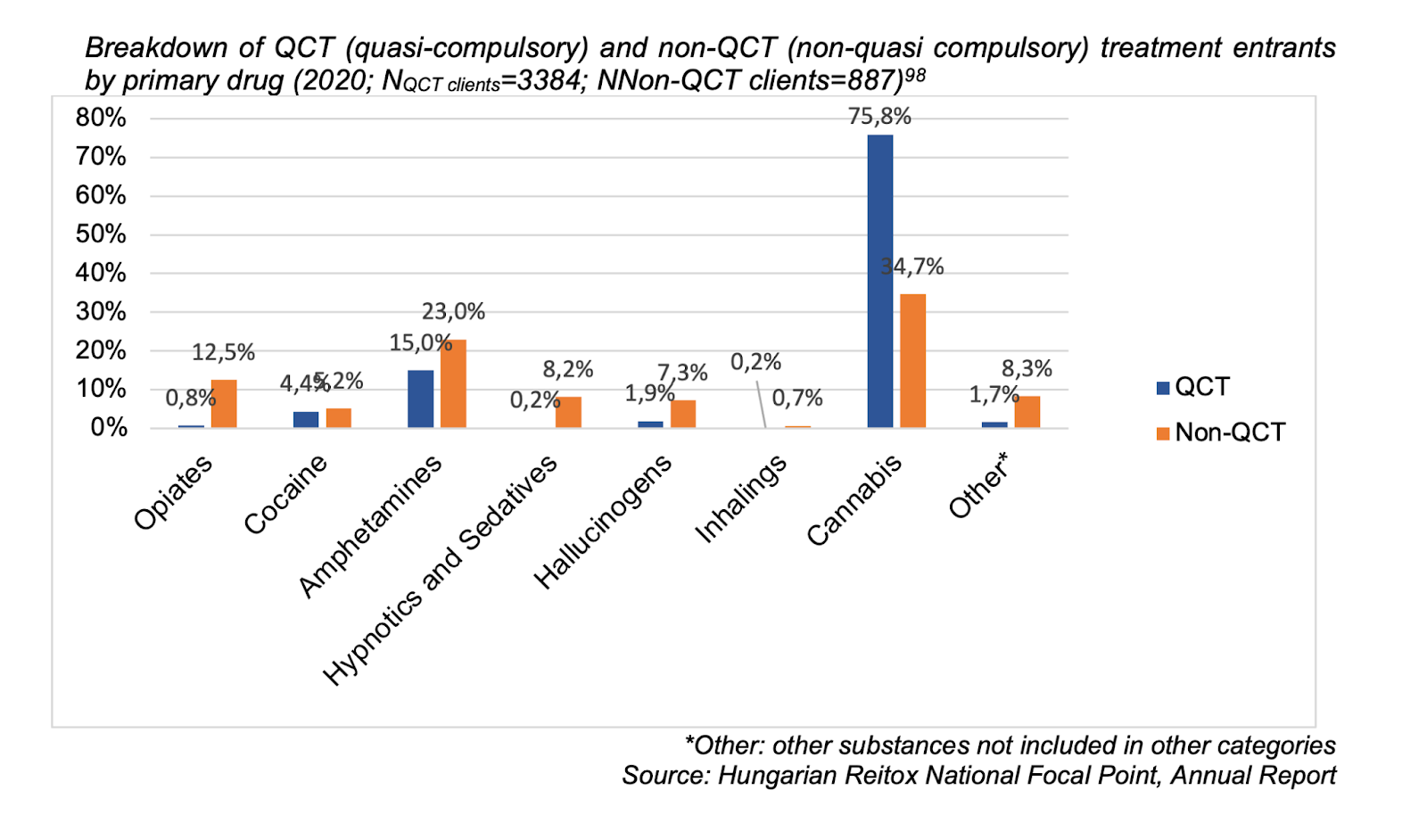
While there was a substantial increase in cannabis-related treatment demand between 2016 and 2020, this increase is mainly attributable to the increase in the number of those who entered treatment as an alternative to coercive sanctions. Cannabis use is the main reason for entering treatment for more than 75 percent of the total number of people in diversion, while this proportion is only 34 percent among people entering treatment without criminal coercion. Most people who enter treatment for cannabis use in Hungary are occasional users who have not consumed cannabis in the 30 days prior to entering treatment.
Conclusions about the strengths and weaknesses of the diversion mechanism
The diversion of offenders who possessed small amounts of illicit drugs from the criminal justice system was an important development in the Hungarian drug legislation. There is strong evidence that this is an effective mechanism to achieve its main goal: to provide an alternative to punishment for thousands of young people every year who would otherwise be sentenced by a criminal court. It is also an effective tool to reduce the administrative burden and costs of prosecutors and judges, wasted on the criminalisation of non-violent offenders who commit a victimless crime. There is also some evidence on the positive impact of the quasi-coerced interventions on reducing drug use (however, it is not sure whether this reduction has been sustained after the program ended).
However, there are still a lot of ethical and professional concerns about the diversion to treatment, especially with its recent state, after several amendments.
- Young people diverted from the criminal justice system are still arrested and undergo an often humiliating and traumatising process by being the target of an arrest, a urine drug test, possibly a house search, visits to a probation officer, and other interventions.
- Although a) drug use is a risk taking behaviour, b) prevention and education have benefits in reducing the risks and c) diversion is still better than full criminalisation, this does not justify the use of criminal justice coercion in forcing young people to undergo a health/social intervention. The benefits of attending an educational-preventional program do not legitimise the use of criminal justice coercion in other fields of life.
- It is a bad prioritisation and allocation of resources to invest in coercing thousands of occasional cannabis users into treatment/prevention interventions while voluntary programs and services are often chronically and severely underfunded and understaffed, and people with severe drug problems have low access to live-saving voluntary treatment and harm reduction services.
- Human rights lawyers report that more and more young people are required to pay the costs of the criminal investigation, which they often cannot afford, and this is against the general aim of the mechanism to exempt these offenders from the consequences of criminalisation.
- Although there was a substantial increase in the prevalence of use of novel psychoactive substances, the users of these drugs are not offered the opportunity of diversion and are punished with administrative sanctions.
- There are no alternatives to coercive sanctions to those offenders who committed a non-violent small-level property crime with the intention of feeding their drug habit, although there is international evidence that this can reduce future re-offending.
- There is a lack of knowledge and understanding from police officers about the social, health and human rights aspects of drug use and they are not able to connect offenders with drug problems to relevant services.
- The legal and professional documents on diversion are outdated and do not respond to recent challenges reported by clients and service providers.
- People who live/work abroad but are arrested for a drug offence in Hungary are not able to complete the diversion program either online or at a drug service in their country of residence.
- The timeframe of the diversion scheme is too rigid and does not allow adjusting the program to the specific needs of the clients.
- The funding for alternatives to coercive sanctions is not adequate to ensure the sustainability and quality of these services.
Decriminalisation: the real alternative
Although the diversion from the criminal justice system in Hungary has some benefits, especially when we compare it to the negative consequences of fully enforced criminalisation, it needs significant revisions and amendments.
Decriminalisation of drug use – investing in voluntary care
Our most important recommendation is to introduce the full decriminalisation of the use/possession for personal use of illicit substances, but increase investment in voluntary prevention, treatment, and harm reduction programs. That is, not to impose any criminal sanctions simply for what people put into their own bodies, but to address the underlying social and health determinants of risky behaviours through non-coercive education and support. There is conclusive evidence that these demand and harm reduction programs are the real highly effective alternatives to punishment, not in making society drug-free, but in making it safer and healthier. This is the ultimate alternative to criminal sanctions. There are international good practices to decriminalise drug use, for example in Portugal, where possession offences are assessed by an expert commission, and voluntary help is offered for those who are in need. According to evidence, decriminalisation does not increase drug use but reduces health and social harms.
Law Enforcement Assisted Diversion
As an alternative to the current diversion system, we recommend using alternatives to coercive sanction for people who commit low-level drug distribution, property and other non-violent crimes where the criminal activity stems from unmet behavioural health needs and/or poverty. A good practice to apply is the Law Enforcement Assisted Diversion (LEAD) project in Seattle, US, where police officers are instructed to connect these offenders with trained intensive case managers who can provide crisis response. This includes immediate psycho-social assessment and services to address drug dependence and other health and social problems, including housing.
Recommendations to improve the diversion system
Until the criminal laws are reformed and drug use is decriminalised, we have more immediate recommendations about amending the current system. After reviewing the available evidence on the use of the diversion to treatment scheme in Hungary, decision makers should create a new ministerial decree and new professional guidelines to make the diversion system more fit for purpose. These documents should address the following issues:
- Open up the opportunity to be diverted from the criminal justice system to all substance users, including the users of novel psychoactive substances.
- Make the time framework of diversion more flexible and give more professional autonomy to service providers to decide, based on the initial assessment, what should be the goal, length, and methods used.
- Clients should be involved in planning their diversion treatment and preventive-consulting program as it improves the effectiveness of these interventions.
- Offenders who reside or work outside of Hungary should be given the opportunity to complete the diversion program online.
- The costs of the criminal investigation should not be charged to the offender as it endangers the goals of diversion (this requires an amendment in the Law on Criminal Procedures).
- Training courses and professional consensus-building meetings should be organised regularly between law enforcement officials and social/health professionals who provide diversion services to exchange ideas and build partnerships.
- Training and methodological support should be provided to service providers to ensure the quality of diversion services.
- Adequate, timely, and regular funding should be provided to ensure the sustainability of diversion services.
- Regular monitoring and evaluation of diversion services should be improved.
SOURCES
Dudits D., Jambrik Á., Gáspár G., Törzsökné Góczán E. (2010): Megelőző-felvilágosító szolgáltatás. In: Felvinczi és Kun (szerk.): Szabályozás a célzott és indikált prevenció területén I. 176-225. o. Budapest: Szociálpolitikai és Munkaügyi Intézet.
Felvinczi K., Paksi B., Magi A. and Sebestyén E. (2018) Kutatási beszámoló. Az elterelés keretében végzett megelőző-felvilágosító szolgáltatás tartalmának és közvetlen hatásainak vizsgálata – című kutatás első fázisának eredményei. Magyar Addiktológiai Társaság, Budapest.
Pelle, A. and Dénes, B. (2000) A szigorítás útján. A kábítószer-jogszabályok és a hatályba lépésük óta eltelt egy év értékelése. TASZ, Budapest.
Rácz, J. et al. (2008) How theory is put into practice: the analysis of in-treatment drug users under “treatment alternative to prison” in an outpatient centre in Budapest. Orvosi Hetilap 149 (13): 601-607.
Vitrai J. ed. (2010) Büntetés helyett. A büntetőeljárás alternatívájaként működő elterelés értékelése. L’Harmattan, Budapest.
2020 NATIONAL REPORT to the EMCDDA by the REITOX Hungarian National Focal Point (2021) Budapest.







