
According to data from the Centre for Disease Control (CDC), every day 91 Americans died due to opioid-related overdose in 2015 [1]. Between 2000 and 2015 over half a million people have lost their lives. Opioids can rarely be blamed on their own, in most cases opioids combined with other drugs, most often anti-anxiety benzodiazepines such as Xanax (alprazolam) and Valium (diazepam), lead to the tragedy. The latest CDC data is from 2015 and at that time the end of the epidemic was not even in sight. The problem has reached a point where it is arguably one of the greatest public health issues in the States. Even late night talk show hosts, like John Oliver, are talking about the phenomenon.
Health experts blame the epidemic in part on the overprescription of opioid based painkillers. Between 1991 and 2011, the number of opioid prescriptions in America has increased from 76m to 219m [2]. The most popular substance is the semi-synthetic opioid oxycodone, which is sold under various brand names such as Oxycontin, Oxecta, and Roxicodone. As a good example of just how many opioids are prescribed, pharmacies from the state of Maine have supplied enough opioid based painkillers to supply every citizen of the state for 16 days! Or to put it differently, roughly every 20th citizen has enough opioids for an entire year.
People use opiates to numb their pain, but these drugs also have a respiratory depressant effect (i.e. they slow down breathing). Importantly, the tolerance for the drug’s pain numbing effect builds up quicker than tolerance to its effect on the respiratory system [3].
What can be done to stop the epidemic? Most of the conversations revolve around how to change the guidelines for prescribing these painkillers. It is certainly an important step, but it can only help to reduce future use and is no remedy to people who are already using/abusing these drugs. One solution is medication-assisted treatment. The idea is to replace the troublesome substance with something that has a better safety profile. For example in the context of heroin use, methadone or buprenorphine are commonly used treatments. They are also opioids, but less euphoric than heroin, that can help to abate withdrawal symptoms during detoxification, or as maintenance to help combat cravings.
Marijuana is less addictive than opioids and for all practical purposes you can not overdose on it, but it also has analgesic (painkiller) effects. There is pharmacological evidence between the interplay of the brain’s cannabinoid and opioid system, thus it might be possible to contain opioid use with marijuana [4]. Providing evidence for this possibility, a study based on a nationally representative survey of young adults found that marijuana use was associated with a 55% reduced risk of past year opioid abuse [5]. An exploratory study from San Francisco reported approximately ⅔ of medical marijuana patients used it as a substitute for prescription medicines, however, this study did not investigate what drugs patients substituted with marijuana [6]. Recently a new study from Piper and colleagues followed up this study to figure out what class of drugs medical marijuana patients are substituting [7].
The study took place in New England and was primarily promoted through medical marijuana dispensaries. Patients who purchased products were given information about the study, but participation was voluntary. Participants were directed to an online survey that was designed to figure out whether patients have reduced their intake of medication and, if so, what class of drugs they substituted with medical marijuana. Overall 1513 patients responded to the survey, most of whom were prescribed medical marijuana due to chronic pain (70.4%), post traumatic stress (25.5%), severe muscle spasms (12.2%) and nausea (10.6%).
The sample was ethnically highly homogenous, with 94.8% of the sample identifying as white and composed of mostly educated people. Interestingly most people prefer smoking joints (48.5%) compared to any other form of consuming cannabis (vaporisers 22.3%, edibles 14.3%) and most users preferred indica dominant strains to sativa strains (63.6% vs 36.4%). Participants were also asked about their motivation to smoke cannabis on a scale from ‘0% medical, 100% recreational’ to ‘100% medical, 0% recreational’. The response in the sample was 15.3±0.5% recreational, hence, the motivation was largely medical for the sample.
Of the subset of medical marijuana patients who also used opioid based pain medication (n=215) over ⅔ indicated that they reduced their painkiller intake either ‘slightly’ or by ‘a lot’. This was significantly lower than the number of patients who reduced their antidepressant intake (37.6%). Antidepressant dosing was used as a comparison group, since they are typically not prescribed on an ‘if needed’ basis (unlike painkillers). Patients also reduced their intake of anti-anxiety (71.8%), migraine (66.7%) and sleep (65.2%) medication as well. Figure 1 below summarises the substitution effect of medical marijuana.
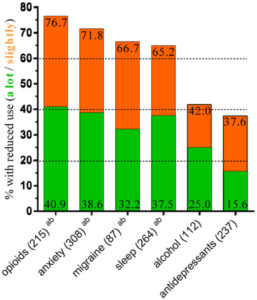
Figure 1: Percent of respondents with a reduction in various classes of medications. Number of patients that regularly used each group of drugs is in parentheses. The numbers on each bar represent the % of people who reduced by ‘a lot’ and overall (bottom/top number).
Researchers also analysed written responses to the question ‘What do you like most or least about medical cannabis?’ Figure 2 below shows a graphical representation of the themes: the larger a word is, the more frequently it appeared among the answers.
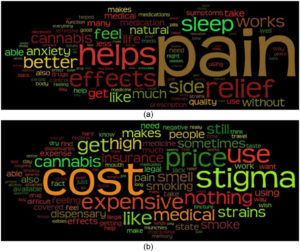
Figure 2: qualitative representation of word frequencies in the responses to the question ‘What do you like most (a) or least (b) about medical cannabis?’.
Whilst the results of the study look promising there are a few caveats that the reader should bear in mind. The study could be criticised for not assessing quantitatively by how much medical marijuana patients decreased their opioid intake. The categories ‘slightly’ and ‘a lot’ from Figure 1 are never precisely defined and as a result it is hard to say whether the decrease has any public health significance.
Similarly the study did not investigate which subset of opioid users substituted their painkillers with medical marijuana. It would be interesting to see if light and heavy opioid users decreased their intake in a similar fashion or not. The substitution effect would be much more valuable from a public health perspective if it could help heavy opioid users to decrease their use.
Also the sample selected is biased in multiple ways. As mentioned earlier the sample was practically all caucasian. Moreover patients were recruited through marijuana dispensaries. It is likely that this self-selected sample was more motivated to reduce their opioid use. Therefore it is possible that the substitution effect is not driven by the pharmacological action of marijuana, but rather it is by psychological factors.
Similarly the study has a cross sectional design that makes causal inferences challenging. As is often emphasised in this blog, there is just no substitute for randomised, double-blind clinical studies. Thus, as a result it can be said that there is a long way until medical marijuana can become an officially recognised ally to fight the opioid epidemic, nonetheless every step towards this direction should be welcomed!
B Szigeti
References:
[1]: https://www.cdc.gov/drugoverdose/epidemic/ (accessed on 3 May 2017)
[2]: https://www.economist.com/blogs/graphicdetail/2017/03/daily-chart-3 (accessed on 3 May 2017)
[3]: Dumas, Emily O., and Gary M. Pollack. “Opioid tolerance development: a pharmacokinetic/pharmacodynamic perspective.” The AAPS journal 10.4 (2008): 537.
[4]: Reiman: Cannabis as a substitute for alcohol and other drugs. Harm Reduct J 6: 35, 2009.
[5] Pisano, Vincent D., et al. “The association of psychedelic use and opioid use disorders among illicit users in the United States.” Journal of Psychopharmacology (2017): 0269881117691453.
[6]: Fattore L, Cossu G, Spano MS, . (2004) Cannabinoids and reward: Interactions with the opioid system. Crit Rev Neurobiol 16: 147–158.
[7]: Piper, Brian J., et al. Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep. Journal of Psychopharmacology (2017): 0269881117699616.







